- March 3, 2023
- By: Dr. Subodh Kamble
- No Comments
ADULTS WITH TESTICULAR PAIN: BE WARY!
As in my last post I discussed a case of child with testicular torsion who came to me as an emergency, similarly I had also seen couple of adults presented with similar complaints. Hence, I am taking this opportunity to discuss it here to show how adults with testicle pain could be different. I had to attend the hospital twice in one day, which is rather unusual in current days and funny thing is that on both occasions it was for over 50 adults complaining of same thing ‘The Testicular Pain’. The adult testicular pain is not the same as the adolescent males (males between age group of 12-18 years). The possibility of torsion or twisted testicle is very low in adults however it should still be taken very seriously.
As soon as I was informed about the 54-year-old gentleman with sudden onset of testicular pain, without losing much time I reached the hospital. The pain had started suddenly about 4 hours ago. This was without any infection, or an injury to that area, and for the first time in his lifetime. Even though I knew that twisting is rare in adults, I wasn’t completely convinced in his case and had strong suspicion of untoward scenario. His examination did not reveal typical findings of the twisting, but the testicle was rather swollen and tender to touch. It was rather dubious situation where some of the things were indicating twisting, whilst some were not. I had to take a call and make my decision. I do not have a very low threshold for scrotal exploration (surgery for twisted testicle) for the adults with pain but I also make my decision on case to case basis and do not apply blanket policy.
In this scenario, on the basis of my clinical judgement, my experience and my knowledge I decided that I would like to operate on the gentleman’s scrotum to make sure he does not have the twisted testicle. I explained my concerns to him, the benefits Vs risks of operating and nonoperating in these circumstances. It is my practice that I never force my decisions on to the patients, but I help them reaching sensible decision through mutual thorough discussion and with patients’ as well as their relatives’ (if present) complete satisfaction. This occasion wasn’t an exception and together we made a decision for operation. In such emergency situations as well as other emergency situations I always take decisions in patient’s best interest, but they are always informed and well consented.
I am glad that I operated on him as he did have a twisted testicle, which I untwisted and was able to save it. He was also happy with the outcome. Not that he needed the testicle very badly as he had already completed his family, but there is psychological impact as well as it can affect production of male hormone Testosterone. Next day he went home and was thankful to me for assessing his situation correctly and intervening at the right time with right decision. It is always satisfying when patients go home with happiness and satisfaction. This feeling is certainly beyond any comparison.
As per one of the South Korean study they found that for 100000 population the rate of twisted testis between age group of 10 to 19 was around 10, but as the age increased the percentage went down and went to 0.1 patients out of 100000 population between age group 50-59. Hence it is uncommon to see twisted testis in this age group however age on its own shouldn’t be considered as an omission criterion for the twisted testicle. If a urologist does not consider the diagnosis and not suspect it, the twisted testicle in older people could cause missed or delayed diagnosis. This certainly not only could jeopardize the chances of saving that testicle but also could end up in severe life-threatening sepsis.
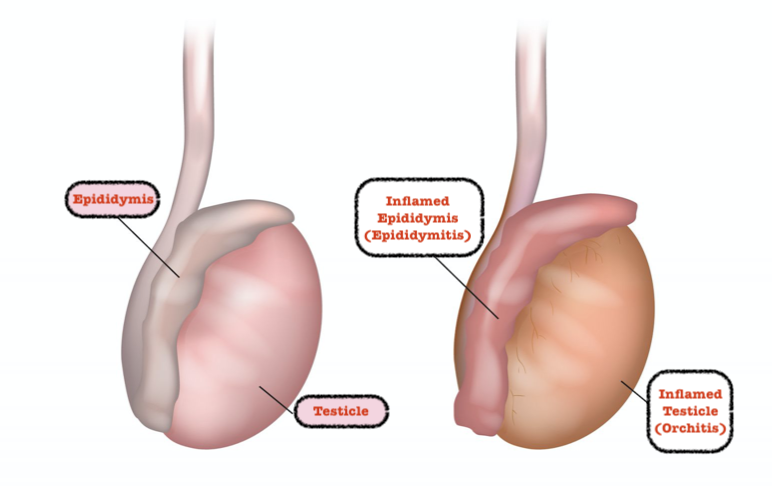
On the same day I was consulted by another gentleman in late 50’s with testicular pain which was going on for 2 days. He also had fever, swelling of one side of his scrotum. Once again, I went to the hospital to see the gentleman who was in pain. His complaints and the examination suggested a possibility of testicular infection called ‘Epididymo-orchitis’. There were other clues confirming my diagnosis. He had urinary symptoms suggesting urine infection, infection was suspicious on urine examination, his blood tests showed raised markers of infection such as white blood cells and blood test called CRP. In such patients an ultrasound scan of the testis should be done to rule out the possibility of testicular or epididymal abscess. Thankfully my patient did not have an abscess, but I had to keep him in the hospital for intravenous antibiotics, which was then changed to oral antibiotics to take at home.
Such two completely opposite testicular pain presentations in one day in adults shows the wide range of possible diagnosis. In adults one has to also make sure that they have ruled out the testicular tumours as 10% patients with testicular cancers may present with pain in the testis. I always take testicular pain very seriously irrespective of patients age and attend them immediately. Depending on presentation I also have low threshold for operating such patients.
Lockdown or no lockdown, when something like testicular pain, which is an emergency, one should attend the hospital and see the urologist as the time could be critical and an important organ could be fighting for its survival!