- March 3, 2023
- By: Dr. Subodh Kamble
- No Comments
COMMONLY WRONG INTERPRETATION OF URO-DYNAMIC STUDY AND DISASTERIOUS CONSEQUENCIES FOR PATIENTS!
As promised in my last post, I am going to share with you some information about the role of urodynamic study, what it is and how one wrong interpretation of this investigation can lead a doctor on to a wrong treatment tract ending up in ruining patient’s life. Since starting my practice in India, I have commonly noticed that urodynamic study carried on a patient was completely misinterpreted with wrong result as well as proposing wrong treatment to the patient. Patients coming to me with urine problems generally have been to three to four Urologists, several investigations carried out and still no relief from their symptoms, leading up to ultimate explanation that there is no treatment for their condition. Such patients come to me with big bunch of files in a hope that I would treat them, I would relieve them from their problems and thankfully I have been able to help my patients to relieve them from several years of suffering with urine leak. This is evident from their remarks, their reviews about me and from their follow ups. Out of many such examples I am choosing the same patient I had discussed previously for the purpose of this article. That young dynamic IT professional lady’s case opened up the pandora’s box of wrong interpretations of an investigation.
She had been suffering from urine leak for 14 years. She consulted several doctors before she consulted me and sadly none of them were able to help her. Her symptoms looked like a mixed incontinence (urine leakage) with bowel problems including faecal leakage. She had severe symptoms of irritable painful bladder. For many years she was consulting gynaecologist abroad (NRI), but no relief and with her years of suffering she decided to consult doctors in India in Ahmedabad, Gujarat. After consulting gynaecologist in Ahmedabad who investigated her and referred her to urologist after her few visits. She then consulted one of the well-known and topmost urologists in Ahmedabad who carried out plethora of investigations including she visited a large corporate hospital.
As previously stated, she was put through unnecessary cystoscopy (telescopic examination of bladder) under general anaesthesia. She was neither explained about the purpose for such test nor doctors discussed the result except telling her that she has urine leakage. Why I would call it as unnecessary procedure is because she was going to need intravesical procedure any ways following her correct diagnosis in order to treat her. During the intravesical treatment one would look inside the bladder any ways hence there was absolutely no point putting her through same procedure twice and putting her through general anaesthesia unnecessary on two occasions. One must not put patients through unnecessary anaesthesia as the general anaesthesia has its own risks and complications. One may think that due to her symptoms there was need to look inside bladder. Agreed! But certainly not without proper treatment. If correct treatment plan was established at early stage, then this procedure was going to be unnecessary.
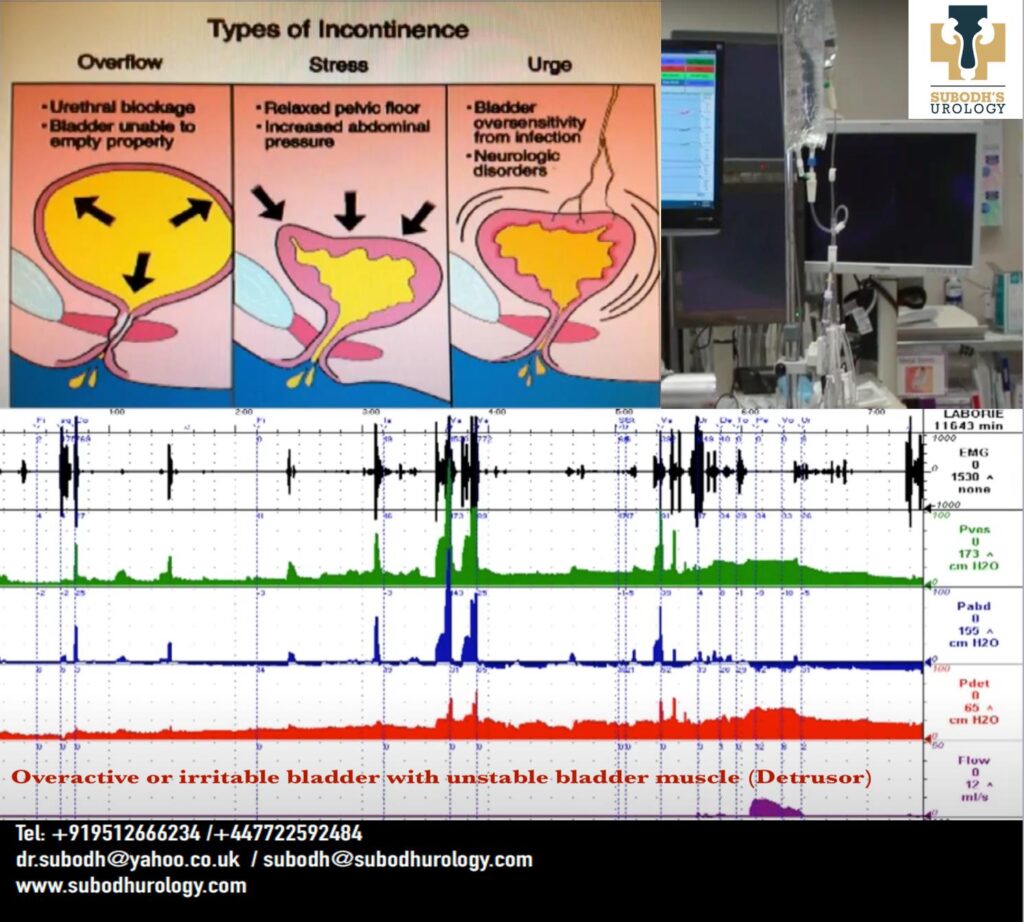
She also had Urodynamic study carried out, which is a functional study to reciprocate symptoms, assist in diagnosis, to outline significant abnormalities and to allow selection of most appropriate treatment. You may appreciate now as to how important it is for the correct interpretation of this test. It involves measurement of urine speed and volume and the amount of urine left in the bladder after emptying the bladder. It monitors pressures in of bladder as it fills up, amount of urine the bladder is able to hold, and point of urge to urinate. It measures abnormal contractions or spasms of your detrusor muscle (smooth muscle in the wall of bladder) during filling caused by overactive bladder. It also measures pressure at the point of leakage of urine. A strain by using regular coughing and leak can indicate stress incontinence. A pressure flow study measures the pressure of the bladder required to urinate.
In this lady’s case she wasn’t asked to cough regularly at every minute, neither any leak was documented or possibly seen. The detrusor (bladder muscle) showed clear cut evidence of overactivity but this was missed, and she was told that her bladder muscle is stable. At end of her filling of bladder when she was holding roughly 500 ml in her bladder, she had leak due to urgency, but it was misinterpreted as leak due to stress (weakness of muscles).
As per the International Continence Society (ICS), Detrusor pressure (bladder muscle) in females of 20-40 Cm of water are normal. Blockage to urine is suggested if detrusor pressure at maximum urine flow is above 25 and maximum flow is less than 12 ml/second. Similarly, it can be said that the bladder or detrusor is underactive or weak if detrusor (muscle) pressure at maximum urine flow is below 10 cm of water and maximum flow is less than 12 ml in one second. In this lady’s case her detrusor pressure was 20 and the maximum flow was 18 ml/second, but she was still told that her bladder muscle is weak, and she may need to use catheter to empty bladder! She was then prescribed a medication called Mirabegron for the same and was asked to have a trial for one week of this medicine. I found it bizarre as she had already used this medicine for nearly 2 years without any relief from her symptoms. This medicine takes at least 2 weeks to show effects and it is given for irritable bladder and not the underactive bladder as they had suggested she had. Their own interpretation was that she had stable bladder with no element of irritable bladder hence it made no sense to prescribe it, that too only for a week.
As you can appreciate now that how every part of the test was misinterpreted, and from the test the urologist made a diagnosis of stress incontinence. Stress incontinence is a leakage of urine on cough, sneeze, laughing or even jumping. It happens due to weak pelvic floor muscles, or weak sphincter (valve at the opening of bladder). Based on their wrong interpretations of the urodynamic test and their own assessment the urologist planned a major surgery for her involving two surgeons (Urologist and a General surgeon). The urologist explained her that he would make a big cut on her lower tummy, go in, go under the bladder and lift it up. The general surgeon was to repair her anal sphincter (back passage valve) which was completely unnecessary. They had told her that she would be required at least 15 days hospital stay. I treated her by telescopic surgery in about 30 minutes surgery and two days hospital stay with only about 25% of the bill they had quoted her.
I frequently see these kinds of wrong interpretations of Urodynamic study my patients bring to me. If you remember from one of my previous topics of “Interesting debate of mind Vs coronavirus” about my patient Rekhaben was also one such example.
The NRI lady didn’t go ahead with surgery in Ahmedabad but instead came to consult me, had scar less operation and went back home completely cured from her problems. This was possible through my correct interpretation of her investigations. I re-interpreted the urodynamic study (without carrying out new study) that Ahmedabad doctor had carried out. A careful and thorough history taking, and examination is vital to provide patient curative treatment. If she had underwent the proposed surgery by the Ahmedabad urologist, she would have had irreversible damage and she could have had lifetime sufferings and without treatment of her original problems. In fact, that surgery would have made her problems worst. It is always satisfying when I am able to help someone and able to cure them. She was glad that she made timely decision and came to me for second opinion and further treatment.
I always give a lot of emphasis and importance to interpret the investigations correctly as, if you don’t, it can have detrimental effect on patient’s health. I also highlight that doctors should avoid treating and referring to inappropriately trained person. If a doctor doesn’t possess required experience or expertise in that area then they shouldn’t involve themselves in such practice area, if they do then it can ruin someone’s life! After all we are dealing with lives and livelihood of a human.
MY ADVICE:
• Try to find out or read about the doctor (their experience and expertise) you are seeing for your major problems.
• Ask the doctor about their experience in the area which you are consulting them for.
• If in doubt you can opt for second opinion but make sure you are consulting an experienced and appropriately trained doctor in that particular subspecialty, for example in this case female urology knowledge and training was absolutely paramount.
• Urine leak is always abnormal, hence if noticed see urologist.
• Take blood in the urine extremely seriously and seek immediate medical attention.
• Ask for the details of your investigations your doctor is proposing to do, ask for reasons for carrying out that investigation and the risks Vs benefits. Ideally you should not have to ask a doctor for this as it is part of doctors ethical responsibility to explain you everything before making any decisions about your health.